
Joint Mobilization of the Upper Extremity
| CONTACT HOURS: | 4 Hours |
| CEU: | 0.4 |
| AOTA: |
Domain of OT, OTP, Check Accreditation
|
| NBCOT®: | 5 PDUs |
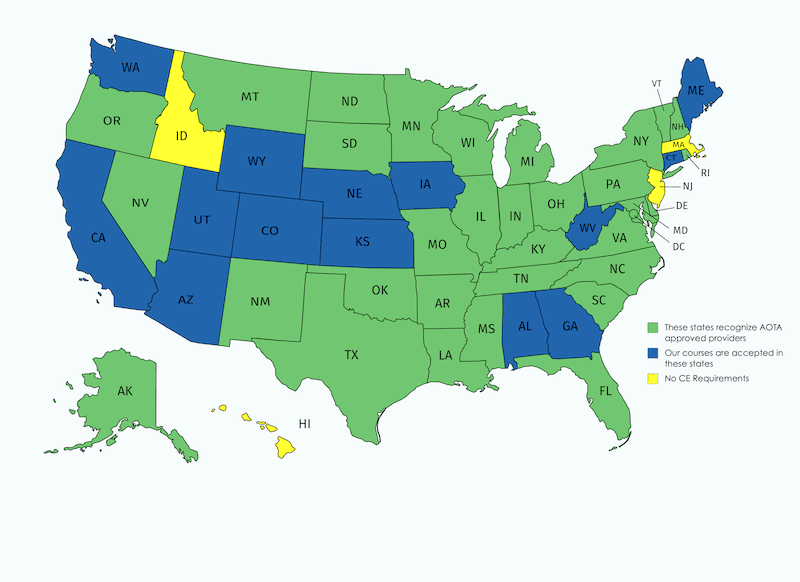
| STATE: |
FL 20-171353 4hrs CA 40-H23 4.8hrs |
This interactive course is in movie format. This course is excellent for occupational and physical therapists, COTA’s, and PTA’s that want to learn the art of joint mobilization.
PDF Course Manual Included.
Buy Now
$155.99
Hand Therapy Certification
This course is accepted by the Hand Therapy Certification Commission towards re-certification.

Description
*University & multi-center Licensure available upon request; all courses single user only
*Watch on your idevices, smart phones, tablets and MORE
Domain of OT, Occupational Therapy Process
This interactive course is in movie format. This course is excellent for occupational and physical therapists, COTA’s, and PTA’s that want to learn the art of joint mobilization. You will learn mobilizations techniques up close and learn how to make stiff joints move. Watch, rewind and re-watch. This feature allows you to “take the instructor home with you”. This is a mixed learning level course.
Note: This mixed learning level online movie course provides conceptual preparation to seek additional training, and does not provide you a mentored hands-on skills session. Please seek additional experience, with a mentor, to perform hands-on skills. Upon Successful completion of the examination (80%) your certificate will be available in your account Dashboard.
Objectives
-
- Review precautions and contraindications for joint mobilization
- Review joint mobilization techniques that promote good body mechanics and mechanical advantages
- Introduce joint mobilization skills that will insure accuracy and consistency
- Understand the type of joint you are mobilizing
- Introduce joint mobilization skills that will insure effective and efficient treatment
Outline
- Introduction
- Definition-skilled passive movement of a joint
- Overview
- One “tool” in the therapists “tool box”
- Used only after determined by a thorough evaluation that joint mobilization is needed
- More effective if combined with an active rehabilitation program
- Indications
- Joint hypomobility
- Contraindications
- Unstable joint
- Hemiarthrosis-bleeding in the joint
- Healing fracture-involved or adjacent joint
- Acute inflammation
- Bony disease
- Cancer
- Infection
- Precautions
- Muscle guarding
- Osteoporosis
- OA
- RA
- Hypermobile joint
- Swelling and inflammation
- Fracture not fully healed or undiagnosed
- Anatomy & physiology-know what you are mobilizing so you have an expectation (patient also) as to what is going to happen
- Joints
- Type
- Saddle (i.e. carpometacarpal jt. of the thumb)
- Gliding (i.e. intercarpal jts.)
- Ball and socket (i.e. glenohumeral jt.)
- Pivotal (i.e. radiohumeral jt.)
- Hinge (i.e. humeroulnar jt.)
- Ellipsoid (i.e. metacarpal phalangeal jts.
- Bicondylar (i.e. interphalangeal jts.)
- Cartilage
- Concave surface cartilage is more dense around the periphery
- Convex surface cartilage is more dense in the center
- Cartilage is bloodless
- Concave-Convex principle
- Concave on Convex
- Convex on Concave
- Instances where concave-convex principle does not apply
- Type
- Ligaments and Capsule
- Ligaments contain kinesthetic receptors
- Ruffini endings
- Golgi tendon receptors
- Pacinian corpuscles
- Capsule tissue is fibrous and is interlaced with ligaments and tendons
- Ligaments have great tensile strength
- Ligaments contain kinesthetic receptors
- Joints
- Osteokinematics
- Classical motions (i.e. flexion, extension, pronation, supination, etc.)
- Athrokinematics
- Movement relationships within the joint (i.e. glide, spin, roll, etc.)
- Examination-General Principles
- Avoid assumptions; start from scratch and do not assume anything
- Avoid the “I give you a hammer you look for a nail-syndrome.”
- Thorough
- Examination format should include
- Subjective-interview and intake information (see syllabus)
- Examination format should include
- Motion
- Active/Passive
- End feel
- Quality
- Absolutes
- Evaluate involved and uninvolved sides
- Evaluate before and after treatment
- Avoid assumptions; start from scratch and do not assume anything
- Treatment General Principles
- Prepare the patient
- Relaxed
- Supported
- Clear instructions on what to do, what not to do, and what to expect (i.e. pressure, pulling)
- Prepare yourself
- Wide base of support
- Set up in gravity assist position whenever possible
- Firm relaxed hold, not tense
- Accuracy
- Forearm alignment to help guide therapists� direction of force
- Palpate during the mobilization with stabilizing hand
- Observe proximal- when movement begins, you are moving something else and therefore becoming less accurate
- Technique
- Slack skin
- Use pads of fingers, not tips
- Energy conservation/joint protection methods
- Distractions
- Glides
- Tilts
- Rotations
- Mobilization grades
- Grade I
- Grade II
- Grade III
- Grade IV
- Tip on how to determine range and grade
- Stabilization hand compared to mobilization hand
- Prepare the patient
- Joint Mobilization
- Shoulder Complex
- Sternoclavicular joint
- Evaluation
- Treatment
- Posterior glides
- Inferior glides
- Acromioclavicular joint
- Evaluation
- Treatment
- Anterior glides
- Posterior glides
- Scapulothoracic joint
- Evaluation
- Treatment
- Superior glides
- Inferior glides
- Medial glides
- Lateral glides
- Distraction
- Glenohumeral joint
- Evaluation
- Treatment
- Lateral distraction
- Posterior glides
- Anterior glides
- Inferior glides
- Elbow
- Radiohumeral joint
- Evaluation
- Treatment
- Distraction
- Approximation
- Humeroulnar joint
- Evaluation
- Treatment
- Distraction
- Valgus tilt
- Varus tilt
- Radiohumeral joint
- Forearm
- Proximal radioulnar joint
- Evaluation
- Treatment
- Anterior glides (radius on ulna)
- Posterior glides (radius on ulna)
- Distal radioulnar joint
- Evaluation
- Treatment
- Distractions
- Approximations
- Anterior glides
- Posterior glides
- Outward roll
- Proximal radioulnar joint
- Wrist
- Intercarpal joint
- Evaluation
- Treatment
- Anterior glides
- Posterior glides
- Radiocarpal joint
- Evaluation
- Treatment
- Medial glides
- Lateral glides
- Anterior glides
- Posterior glides
- Ulnocarpal
- Evaluation
- Treatment
- Ulnomeniscotriquetrial glide
- Midcarpal joint
- Evaluation
- Treatment
- Medial glides
- Lateral glides
- Anterior glides
- Posterior glides
- Carpal metacarpal joints (2-5)
- Evaluation
- Intercarpal joint
- Thumb
- CMC
- Evaluation
- Treatment
- Medial glides
- Lateral glides
- Anterior glides
- Posterior glides
- Distraction
- Rotations (supination/pronation)
- Metacarpal phalangeal joint
- Evaluation
- Treatment
- Medial glides
- Lateral glides
- Anterior glides
- Posterior glides
- Medial tilts
- Lateral tilts
- Rotations (supination/pronation)
- CMC
- Fingers
- Metacarpal phalangeal joints
- Evaluation
- Treatment
- Medial glides
- Lateral glides
- Anterior glides
- Posterior glides
- Medial tilts
- Lateral tilts
- Rotations (supination/pronation)
- Metacarpal phalangeal joints
- Fingers and thumb
- Interphalangeal joints
- Evaluation
- Treatment
- Anterior glides
- Posterior glides
- Medial tilts
- Lateral tilts
- Anterior-posterior unicondilar glides
- Interphalangeal joints
- Sternoclavicular joint
- Shoulder Complex
Discounted Add On Item(s) Available with this Product

Marc received his B.S. in Occupational Therapy from the University of Missouri-Columbia. He is currently the lead hand therapist at St. John’s in Springfield, MO. He provides comprehensive hand therapy and industrial rehabilitation-related services and is a mentor to other therapists’ on hand therapy issues. He has been teaching for the past 10 years and practicing hand therapy for the past 23 years. He has taught courses on fractures, joint mobilization, arthritis, cumulative trauma, workplace injury, and other hand therapy topics.
5 reviews for Joint Mobilization of the Upper Extremity
You must be logged in to post a review.

- Participants have one year to access the CEU course and exam to obtain CEUs.
- NBCOT® is a registered trademark of the National Board for Certification in Occupational Therapy, Inc. and does not promote or endorse our specific courses, services or training.
Treatment2go is an AOTA Approved Provider of professional development. PD approval ID #3397. This distance learning-independent activity is offered at 0.4 CEU’s, intermediate, foundational Knowledge. The assignment of AOTA CEU Does not imply endorsement of specific Course content, products, or clinical Procedures by AOTA.




Shannon OTR/L,CHT –
This is a great course. One of the better courses I’ve bought online. Mr. Allen demonstrates all UE mobilizations with commentary on body/hand positions that flows nicely. The question session at the end offers additional information regarding convex/concave rule, precautions and a couple of case studies.
Kenny D. Maynes –
Maybe more advanced then I expected. Work outpt and SNF. Looking for course’s for contracture management/ROM etc dealing with, elbows, hands(in general,not going through ever single finger), wrist, shoulder.
Kerstin Waltz OTR/L –
The course material is very helpful and thorough. I like it very much. I can practice whenever I want to. It is also very helpful in teaching students and coworkers.
Gretchen Proctor OTR/L CHT –
Great information. Very well presented. I think that with a Joint Mob course, I need to have more hands on experience and hands on feedback. The information is great to have though, and I feel I got a lot from the course.
Elsa Escobedo OTR –
It was very well organized and helpful. I will continue to review it and learn more each time.
Thank You